

Polymerization of hemoglobin-S (HbS) in the deoxy conformation shortens the lifespan of sickle red blood cells and promotes intravascular and extravascular hemolysis. When sickle red blood cells are lysed intravascularly, HbS is released into the vascular space where it can consume nitric oxide and be oxidized to higher oxidative forms. During these reactions, ferric (Fe3+) HbS is formed, which readily releases heme. The released heme can activate the innate immune pattern recognition receptor toll-like receptor 4 (TLR4) on endothelium, leading to P-selectin expression, NF-ĸB activation, and microvascular stasis in sickle cell disease (SCD) mice with implanted dorsal skin-fold chambers (DSFCs). Heme-induced TLR4 signalling and stasis are blocked by administering hemopexin with the heme.
Plasma hemopexin has the highest binding affinity for free heme, rendering it relatively nonreactive and delivering it safely to the liver for endocytosis and degradation by heme oxygenase-1 (HO-1). Due to chronic hemolysis, hemopexin levels are depleted in SCD patients and mice.
We previously reported that intravenous hemopexin induces hepatic HO-1 activity and inhibits ongoing, spontaneous stasis in the venules of SCD mice for up to 48 hours. Inhibition of HO-1 activity with tin protoporphyrin (SnPP) and the administration of carbon monoxide (CO) to SnPP-treated mice demonstrated that HO-1 and its reaction product CO play important roles in the protection against stasis. In the current studies, we asked the question how much of the hemopexin-mediated protection is due to preventing heme activation of TLR4 signalling versus induction of HO-1 and CO production. We wondered if hemopexin complexed with heme would be as effective as hemopexin alone in treating a vaso-occlusive crisis (VOC) induced with hemoglobin heme.
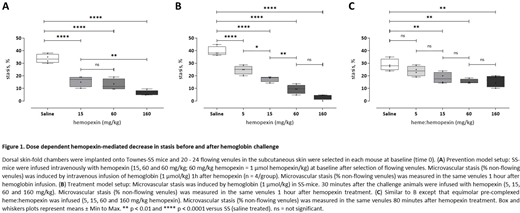
First, in a stasis prevention model, we intravenously administered different doses of hemopexin in Townes SCD mice with a DSFC one hour prior to a hemoglobin challenge. Briefly, anesthetized mice were placed on an intravital microscopy stage, and 20-24 flowing subcutaneous venules were selected and mapped. After baseline selection of flowing venules and one hour after administration of different doses of hemopexin (0 - 160 mg/kg body weight), microvascular stasis was triggered by infusing hemoglobin (1 µmol/kg). The same vessels were re-examined for stasis (no flow) and percent stasis was calculated. Our results show that hemopexin effectively reduced stasis in a dose responsive manner when delivered one hour prior to the hemoglobin challenge (Figure 1A).
Second, we evaluated hemopexin in a VOC acute treatment model by infusing various doses of hemopexin 30 minutes after the intravenous hemoglobin challenge. We found a dose-dependent effect of hemopexin to reduce and resolve microvascular stasis during an acute VOC one hour after hemopexin infusion (Figure 1B). We obtained similar results after inducing stasis with lipopolysaccharide (LPS) or hypoxia-reoxygenation in place of hemoglobin challenge.
Third, we evaluated equimolar hemopexin-heme complexes in a VOC acute treatment model by infusing the same doses of hemopexin-heme 40 minutes after the intravenous hemoglobin challenge (1 µmol/kg) to further elucidate the effects of heme scavenging versus HO-1 induction. Our results showed a striking, dose-dependent reduction in stasis, albeit to a detectably lower degree than hemopexin free of heme (Figure 1C).
In summary, hemopexin has a dose-dependent effect to prevent and treat vaso-occlusion induced in a mouse model of SCD by hemoglobin, LPS, and hypoxia-reoxygenation. This effect is partially replicated by hemopexin pre-complexed with heme, suggesting that the beneficial effect is not limited to clearance of circulating heme and prevention of TLR4 signalling. The partial effectiveness of hemopexin-heme complex is consistent with our prior published data implicating CO generation by HO-1 as playing a role in the relief of vaso-occlusion by hemopexin.
We conclude that hemopexin shows promise for the treatment of VOC. Additional experiments are needed to clarify the activity of hemopexin in clearance-dependent and -independent mechanisms of resolution of vaso-occlusion. Clinical trials of hemopexin are warranted to evaluate its safety, tolerability and potential efficacy in relieving vaso-occlusive pain crisis in patients with SCD.
Gentinetta:CSL Behring: Current Employment. Vercellotti:CSL Behring: Research Funding. Kato:CSL Behring AG: Current Employment. Brinkman:CSL Behring: Current Employment. Zuercher:CSL Behring AG: Current Employment. Belcher:Mitobridge-Astellas: Consultancy, Research Funding; CSL Behring: Consultancy, Research Funding; Hillhurst Biopharmaceuticals: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal